How ScienceSoft Builds Interoperability Into Healthcare Software Ecosystems
We make your systems talk — and keep them talking. By designing interoperability into the architecture (FHIR/USCDI, SMART on FHIR, HL7, DICOM) and enforcing audited, encrypted data flows, you get real-time, vendor-neutral data exchange that stands up to HIPAA, Cures Act, and TEFCA.

Interoperability Risks Driven by Vendor Practices and How We Avoid Them by Design
What blocks interoperability isn't always technology; often it's flawed software vendor decisions. Below, we outline the most damaging vendor practices that not only disrupt healthcare data exchange but also compromise care delivery, inflate budgets, and expose organizations to avoidable legal risks.
We'll also highlight an interoperability-by-design, compliance-anchored approach that ensures integrations don't become a healthcare provider's weak spot.
|
|
What goes wrong |
How we make a difference |
|---|---|---|
|
Deliberate restriction of data exchange to enforce vendor lock-in
|
Many off-the-shelf EHRs and healthcare software platforms impose barriers to data exchange. For example, they may expose read-only or throttled APIs, omit key data fields, or limit access throughput, despite regulatory clarity against such tactics. These constraints drive up the cost and complexity of integrations, trap organizations in vendor ecosystems, and leave data fragmented across silos. |
Our custom software architectures are free of hidden integration barriers.
|
|
Integrations treated as an afterthought
|
In many healthcare software projects, integrations are treated as a secondary concern. They are implemented reactively (in response to requests) or late in development, sometimes post-MVP. The result is ad hoc integrations often relying on data polling, flat file exports, or generic middleware. They are fragile and often fail under real-world workloads, scale, or stricter compliance demands. |
We define integration logic during early-stage solution design, before features are built.
|
|
Compliance gaps in integration design
|
Custom software vendors often design integration logic blind to compliance requirements. Missing access controls, poor encryption practices, unlogged system interactions, or shared service accounts can expose PHI and violate HIPAA and other regulations. In cross-system integrations, when security responsibilities are blurred, audit trails are often incomplete or missing. As a result, covered entities face data breach risks and are forced to add necessary controls after deployment, under regulatory pressure. |
We treat integration points as compliance-controlled zones, not just technical utilities. From the API level up, we enforce HIPAA, HITECH, and other relevant regulations.
|
|
Insufficient validation of data exchange
|
In healthcare projects, integration testing is often deprioritized or excluded from the scope entirely. E.g., vendors only validate the fact of connection (message received) without verifying data completeness, field mapping, or impact on workflows. As a result, data gaps, semantic mismatches, or process disruptions surface only after go-live, requiring costly fixes under real-world pressure. |
We verify every layer of integration during system testing.
|
ScienceSoft's System-Level Approach to Healthcare Interoperability
How we architect interoperability into every system
In every healthcare software project we deliver, interoperability is embedded into the system architecture. Below, we describe how we build scalable, standards-based integration capabilities that remain robust across evolving regulations and workflows.
![]()
Standards-based data modeling
- We use HL7 FHIR R4 or R5 as the primary data model and incorporate relevant USCDI subsets to support nationwide health data exchange.
- We link data elements early to standard vocabularies (SNOMED CT, LOINC, RxNorm, ICD-10, CPT, etc.). This prevents mismatches across systems and shortens interface mapping time.
Why it matters:
Sharing health data using interoperability standards helped avoid over 5.8 million duplicate imaging orders in just one year (2024), within Epic's network alone.
![]()
Write-enabled APIs
- Our custom APIs are based on SMART-on-FHIR, secured with OAuth 2.0 and OpenID Connect, and support bi-directional data flow.
- They can support full CRUD operations and real-time data exchange between the client’s system and any external or internal apps. This eliminates data silos and supports instant updates for workflows such as appointment scheduling.
Why it matters:
A 2024 US national survey found that 47% of digital health companies see high EHR API access fees as the main obstacle to interoperability.
![]()
Dedicated interoperability layer
- We design and implement a dedicated integration layer, often including an API gateway and event bus, to decouple systems and isolate core logic from integration flows.
- For simpler setups, we may use direct custom APIs or middleware. Each option is tailored to meet specific integration volume, fault tolerance, and update frequency requirements.
Why it matters:
A 2025 Forrester study showed that using centralized integration layers instead of direct point-to-point wiring speeds up healthcare app deployment by 50%.
![]()
Security-by-design for every interface
- All APIs use TLS encryption and access tokens with short, configurable expiry periods, aligned with each client’s risk model and security requirements.
- All interface activity is logged and can be forwarded to the client’s SIEM or a custom monitoring setup to enable anomaly detection and audit trails.
- Security design aligns with HIPAA and HL7 FHIR guidelines to ensure compliant data exchange at every point of integration.
Why it matters:
Missing audit trails in API layers were among the top HIPAA violations flagged by the HHS's Office of Inspector General (OIG) in 2024 audits.
![]()
Early EMPI and patient-match strategy
- We can configure deterministic (ID-based) and probabilistic (attribute-based) matching at the design stage, storing all relevant identifiers for each patient.
- We can also connect systems to national and regional MPI hubs to support reliable cross-system identity resolution.
Why it matters:
The Black Book research shows that patient ID mismatches cause 35% of claim denials and cost the average US hospital $2.5 million per year.
![]()
Comprehensive interface QA
- All builds are verified against CDC and IHE FHIR criteria to confirm conformance to interoperability standards, with USCDI content checks and HL7 v2/v3 and CCDA validation where applicable.
- Each integration is tested using load simulations scaled to the expected production volume.
- API security testing is included to identify vulnerabilities in authentication, authorization, and data exchange logic before going live.
Why it matters:
A HIMSS report shows that only 6% of healthcare IT leaders feel confident in their test coverage to prevent patient risk, while 76% rank interoperability testing as the top need in automation.
![]()
Governance and data stewardship
- We maintain centralized data dictionaries and version-controlled mapping tables to ensure consistent semantics across systems.
- All interface updates follow structured change-control workflows to avoid hidden edits, semantic drift, and regression risks.
- In long-term engagements, we also establish versioning strategies, define update policies for shared interfaces, and document service-level responsibilities for integration maintenance. This ensures interoperability stays intact as client systems evolve.
Why it matters:
Based on a recent poll, 74% of healthcare leaders face duplicate admin work from data inconsistencies, while 22% aren't confident in the data they use for reporting and making decisions.
How we recover interoperability in fragmented environments
Many healthcare IT ecosystems are burdened by brittle HL7 feeds, proprietary interfaces, and inconsistent terminology layers. We help re-establish interoperability across these fragmented landscapes using modular, non-disruptive approaches that preserve clinical workflows while enabling modern data use.
![]()
FHIR adapters for legacy systems
We build middleware layers that act as FHIR-compatible gateways for legacy systems. These adapters translate modern FHIR-based requests into existing formats like HL7 v2/v3, SQL, or proprietary APIs while leaving legacy code untouched to reduce regression risks. Over time, direct HL7 interfaces can be deprecated to centralize integration logic and decouple business processes from outdated systems.
![]()
Centralized integration and terminology hubs
For projects involving multiple systems, we implement integration engines to streamline message routing and transformation. When needed, we include a terminology server to map custom or local codes to healthcare standards like SNOMED CT, LOINC, RxNorm, and ICD-10. This architecture reduces long-term maintenance costs and ensures consistent data exchange.
![]()
Data consolidation for healthcare analytics
We can build a healthcare data warehouse consolidating clinical and operational data from systems like EHR, LIS, RIS, and claims modules using ETL/ELT pipelines. It provides secure, HIPAA-compliant storage with role-based access and supports standard data formats such as FHIR and OMOP. The platform enables real-time analytics, BI integration, and predictive modeling, and can be deployed in the cloud, on-premises, or hybrid infrastructures.
![]()
Safe dual-run interface migration
When replacing outdated interfaces, we follow a dual-run approach where newly developed integrations operate in parallel with legacy ones. Traffic is switched gradually in small segments, with rollback options at each stage to prevent service disruption. All transformations are validated using synthetic data and real-world edge cases to ensure accuracy and continuity throughout the migration process.
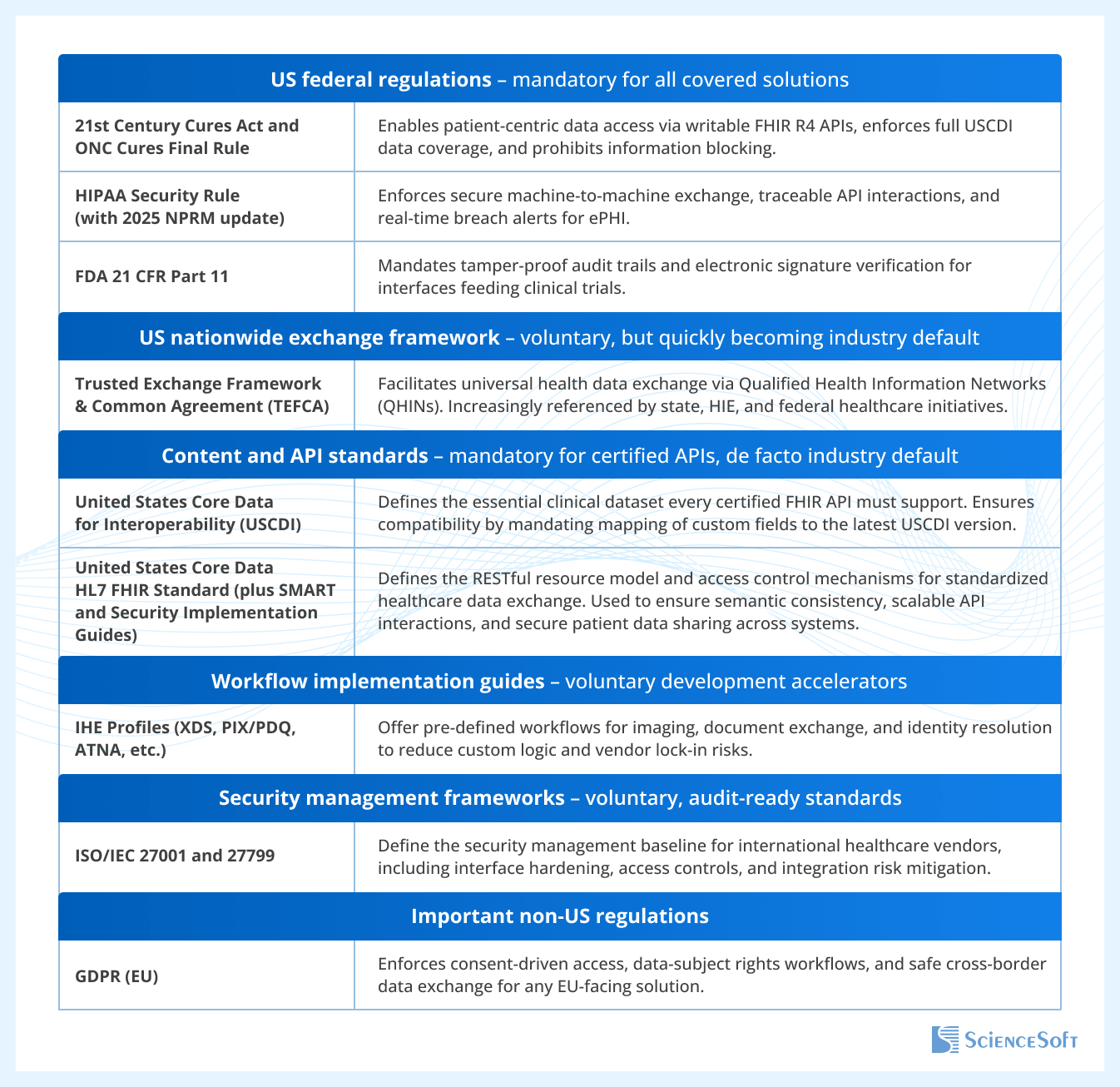
Regulatory foundations of our interoperability practices
These are the key frameworks that shape our integration approach, which ensures compliance, audit readiness, and vendor neutrality across all care settings.